|
|
|
Case #11
|
Typical Clinical Presentation:
|
|
A 12-year-old boy presented with a short history of pain in his thigh.
|
|
|
|
Characteristic Radiological Findings:
|
|
|

|
-
Plain radiograph demonstrates a well-defined, symmetric, expansile, intramedullary lytic lesion of the proximal femur.
|
|
Above findings are common with benign, slowly growing lesions. In this case, the location and symmetric,
expansile growth pattern are very important diagnostic clues. Note that there is no cortical disruption.
|
|
|
|
Pathological Findings: :
|
|
|
|
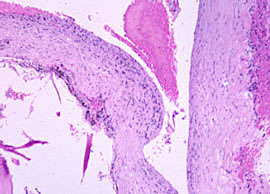
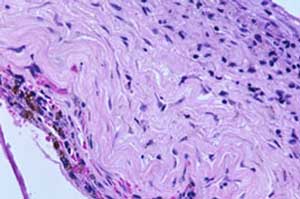
-
The specimen was labeled "cyst wall" and consisted of scant fragments of rubbery white-gray tissue.
Microscopic examination showed bland fibrous tissue with sparse inflammatory infiltrate,
hemosiderin-laden macrofages, and occasional osteoclast-like multinucleated giant cells.
|
|
|

|
- Low magnification, additional
|
|
|
|
|
|
|
Diagnosis: Solitary Bone Cyst (SBC)
|
|
Salient Points::
|
-
Solitary bone cyst is relatively common, non-neoplastic lesion, which typically occurs in the
skeletally immature patients, in the first and second decades of life (80% of cases).
It is usually a unicameral cyst, which does not have an epithelial lining (hence not a true cyst)
and is filled with serous fluid.
-
Location. About 80% of cases are diagnosed in two locations: humerus and proximal femur.
In the long bone, SBC characteristically involves the metaphysis and diaphysis. Other possible
skeletal sites are the ilium, talus, and calcaneus.
-
Differential Diagnosis. You should be aware of the cystic nature of the lesion (ask the surgeon! -
to his eye, the lesion is a cavity filled with clear fluid) This will help you to avoid misdiagnosis
of SBC as a solid lesion.
-
Clinical Behavior. SBC is a benign, slowly growing lesion with recurrence rate of approximately
15%. Pathologic fracture is a common complication. Rare cases of secondary malignancy (chondrosarcoma)
have been reported
Available publications for the topic:
Solitary Bone Cyst
|

