|
|
|
|
|
Case #12
|
Typical Clinical Presentation:
|
|
A 17-year-old male presented with a slowly enlarging, painful lesion of the right clavicle.
|
|
|
|
Characteristic Radiological Findings:
|
|
|

|
-
Plain radiograph reveals a circumscribed, loculated, radiolucent lesion producing blowout expansion
of the bone.
|
|
|
|
Pathological Findings: :
|
|
|
|
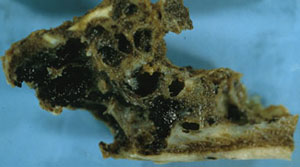
-
Gross photograph shows a spongy, expansile lesion containing multiple,
blood-filled cavities of varying sizes.
|
|
|
|
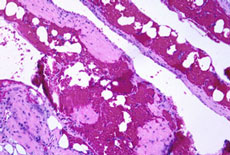
-
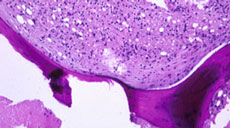
Low-power view demonstrates blood-filled cystic spaces without recognizable epithelial lining.
|
|
|
|
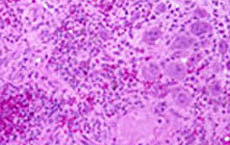
-
The septa are composed of vascular fibrous tissue containing multiple osteoclast-like giant cells,
inflammatory cells and extravasated RBCs.
|
|
|
|
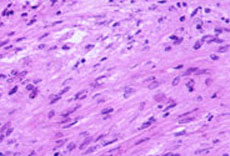
-
High-power view shows uniform, but mitotically active stromal cells. However, no atypical mitoses were identified.
|
|
|
|
-
The periphery of the lesion shows "pushed down", curved trabeculae of pre-existing lamellar bone.
|
|
|
Diagnosis: Aneurysmal Bone Cyst (ABC)
|
|
Salient Points::
|
-
Aneurysmal Bone Cyst (ABC) is a rapidly growing, locally aggressive, intramedullary,
vascular lesion, which characteristically produces blowout expansion of the affected portion
of the bone. ABC can be primary (de novo) or secondary. Secondary ABC may develop in
a pre-existing benign lesion such as chondroblastoma, chondromyxoid fibroma, giant cell tumor, and fibrous dysplasia,
or be superimposed on a malignant tumor (osteosarcoma).
-
Although ABC can occur at any age, the majority of patients are younger than 25 years.
-
ABCs are unique among bone tumors in their almost uniform skeletal distribution and ability to spread
to the adjacent bones and across the joint spaces (Dorfman HD, Czerniak B. Bone Tumors, 1998).
Remember that it is a common lesion in the spine. In a long bone, ABC is usually centered in the metaphysis.
-
Differential Diagnosis. In diagnosis of ABC, correlation with clinical and radiological data is essential.
Remember that secondary ABCs are common. Therefore, you should examine the entire curettage
specimen to search for evidence of a pre-existing lesion. The nature of that lesion, not the secondary cystic change,
determines the clinical behavior. Underlying giant-cell tumor is suggested by the epiphyseal location in the knee
area of a skeletally mature individual. The epiphyseal ABC in a teenager or a tarsal bone ABC suggests a
chondroblastoma as an underlying lesion. Teleangiectatic variant of osteosarcoma may be extremely difficult to
differentiate from an ABC, especially if the latter has "aggressive" radiological features. However, keep in mind that
teleangiectatic osteosarcoma is a high-grade malignancy, and should have foci of sarcomatous stroma with markedly
atypical cells, numerous mitoses and atypical mitoses. The presence of "malignant osteoid" is another feature
distinguishing osteosarcoma from a benign lesion.
Available publications for the topic:
Aneurysmal Bone Cyst
|
|
Selected References::
|
-
Martinez V, Sissons HA: Aneurysmal bone cyst. A review of 123 cases including primary lesions
and those secondary to other bone pathology. Cancer 61:2291, 1988
-
Bertoni F, Bacchini MD, Capanna R, et al: Solid variant of aneurysmal bone cyst. Cancer 71:
729, 1993
|
|
|

