|
|
|
Case #13
|
Typical Clinical Presentation:
|
A 45-year old female presented with increasing pain and swelling around the knee.
She mentioned that the symptoms had progressed over a 4-month period.
-
Age of the patient is an important diagnostic clue. If a pathologic fracture is excluded,
pain and swelling imply active growth of the lesion.
|
|
|
|
Characteristic Radiological Findings:
|
|
|
|
-
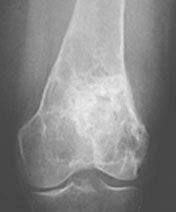
Plain film demonstrates a large, lobulated, ill-defined lesion centered in the distal femoral metaphysis.
There is endosteal scalloping and periosteal thickening. Central stippled and "ring and arc" calcifications
are apparent and are typical of cartilaginous matrix. Small radiolucent areas are seen at the periphery of the lesion.
|
|
These are the features of a locally aggressive, cartilage-producing tumor.
The size of the lesion and the presence of radiolucent foci are very suggestive of malignancy.
|
|
|
|
Pathological Findings: :
|
|
|
|
-
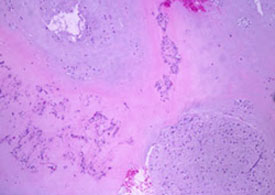
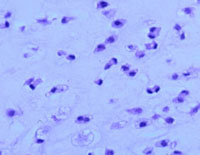
Low magnification shows a moderately cellular, lobulated cartilaginous tumor.
|
|
|
|
-
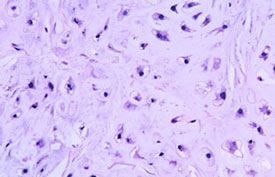
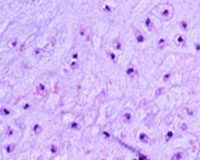
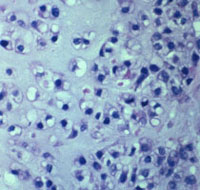
High-power view shows scattered plump, moderately pleomorphic chondrocytes.
Binucleated cells are present. Mitotic rate averaged 1 per 10 hpf.
|
|
|
Diagnosis: Chondrosarcoma, low-grade (Grade 2)
|
|
Salient Points::
|
-
Chondrosarcoma is a malignant, cartilage-producing tumor, which unlike most other primary bone tumors,
tends to occur in the older age group (30-50 years) and is extremely rare in children.
When it does occur in children, it is almost always of a high grade (Grade 3). The majority of
chondroid tumors in children and adolescents are chodroblastic osteosarcomas, not
chondrosarcomas.
-
Chondrosarcoma is the second most common primary malignant bone tumor after osteosarcoma.
-
There are several variants of chondrosarcoma which differ by their location and histologic
subtype. Sometimes, chondrosarcomas are subdivided into primary and secondary to indicate whether they have arisen in a pre-existing benign lesion. Secondary
chondrosarcoma may develop at the sites of radiation osteitis and Paget's disease. Some benign bone lesions
(osteochondroma, enchondroma, fibrous dysplasia) may undergo malignant transformation to a chondrosarcoma.
-
Location. Unlike benign cartilaginous lesions, chondrosarcoma has predilection for the trunk bones including
the pelvis (particularly, ilium), the ribs, and scapula. It is also common in the long bones such as the femur and humerus.
-
The aggressiveness of chondrosarcomas can be predicted by their histologic grade.
Grading system is based on three parameters: cellularity, degree of nuclear atypia and mitotic activity.
|
|
|
|
-
Grade 1 (low-grade)
Very similar to enchondroma. However, the cellularity is higher, and there is mild cellular
pleomorphism. The nuclei are small but often show open chromatin pattern and small nucleoli.
Binucleated cells are frequent. Mitoses are very rare. Grade 1 chondrosarcomas are locally
aggressive and prone to recurrences, but usually do not metastasize.
|
|
|
|
-
Grade 2 (low-grade)
The cellularity is higher than in Grade 1 tumors. Characteristic findings are moderate cellular
pleomorphism, plump nuclei, frequent bi-nucleated cells, and occasional bizarre cells.
Mitoses are rare. Foci of myxoid change may be seen. Unlike Grade 1 tumors, about 10% to 15%
of Grade 2 chondrosarcomas produce metastases.
|
|
|
|
-
Grade 3 (high-grade)
Characteristic findings are high cellularity, marked cellular pleomorphism, high N/C ratio,
many bizarre cells and frequent mitoses (more than 1 per hpf). These are high grade tumors with
significant metastatic potential.
|
-
One of the most important diagnostic features of malignancy is infiltrative growth pattern.
Enchondromas usually have well defined borders with no evidence of invasion.
Quite often you will see nodules of enchondroma surrounded by the bone marrow and
reactive bone trabeculae. That should not be mistaken for invasion.
|
|
|
|
-
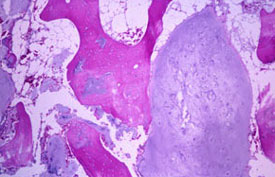
On the contrary, malignant nodules of chondrosarcoma infiltrate between the lamellar bone obliterating the marrow.
Separation of the nodules by fibrous bands would be another feature highly suggestive of malignancy.
|
|
|
-
Prognosis. Survival is related to the histologic grade, location and stage of the tumor. Low-grade
(Grades 1 and 2) tumors are locally aggressive and prone to recurrences, but their metastatic
potential is low. Recurrent tumors may show an increase in grade. High-grade (Grade 3) tumors metastasize to the lungs, skin,
and soft tissues.
- Experimental data:
Studies have shown that p53 overexpression and high Ki-67 proliferation index correlate with clinically aggressive behavior in chondrosarcomas. Recent data suggest that these immunohistochemical stains may be particularly useful for determining the prognosis of patients with Grade 2 chondrosarcomas.
Available publications for the topic:
Chondrosarcoma, low-grade
|
|
Selected References::
|
-
Hasegawa T, Seki K, Yang P, et al: Differentiation and proliferative activity in benign and malignant cartilage tumors of bone. Hum Pathol 26:838, 1995
- Oshiro Y, Chaturvedi V, Hayden D, Nazeer T, Johnson M, Johnston DA, Ordonez NG, Ayala AG, Czerniak B. Altered p53 is associated with aggressive behavior of chondrosarcoma: a long-term follow-up study. Cancer 1998;83(11):2324-2334
- Nawa G, Ueda T, Mori S, et al: Prognostic significance of Ki-67 (Mib1) proliferation index and P53 over-expression in chondrosarcomas. Int J Cancer 69:86, 1996
|

