|
|
|
Case #16
|
Typical Clinical Presentation:
|
A 32-year-old male presented with increasing pain in the knee area.
There were no other physical complaints. His past medical history was non-contributory
and negative for surgery or malignancy.
-
The history of increasing pain is always alarming and suggestive of an aggressive lesion.
|
|
|
|
Characteristic Radiological Findings:
|
|
|

|
-
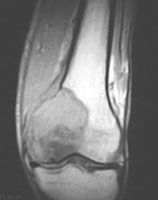
Plain film shows an ill-defined, radiolucent lesion with permeative margins and focal cortical
disruption. The lesion is centered in the distal femoral meta-epiphysis.
|
|
|
|
-
MRI is superior to the plain radiograph in delineating the lesion.
|
|
|
|
Pathological Findings: :
|
|
|
|
-
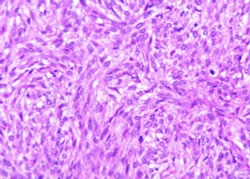
Microscopically, the lesion was composed of interlacing fascicles of mildly pleomorphic,
spindle cells with blunt-ended nuclei and eosinophilic cytoplasm. Average mitotic rate was 3 per 10 hpf.
Geographic areas of necrosis were present.
|
|
|
|
-
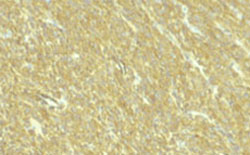
The cells were strongly immunoreactive with SMA (smooth muscle actin) and focally positive for desmin.
|
|
|
Diagnosis: Leiomyosarcoma
|
|
Salient Points::
|
-
Primary leiomyosarcoma of bone is extremely rare with approximately 50 cases reported in the literature.
Our experience includes two cases. Benign leiomyoma of bone probably does not exist
(Helliwell TR. Pathology of Bone and Joint Neoplasms. 1999).
-
Before the diagnosis of a primary tumor can be made, a metastatic lesion must be ruled out.
Common primary sites for leiomyosarcoma include the uterus, gastro-intestinal tract and soft tissues.
-
Differential Diagnosis is usually not extensive and includes fibrosarcoma, MFH, and metastatic spindle-cell carcinoma.
Leiomyosarcoma lacks herringbone or storiform patterns of fibrosarcoma and MFH, stains negative with cytokeratin,
and exhibits strong immunoreactivity with smooth muscle actin and muscle specific
actin (HHF-35). Desmin positivity is seen in only about 50% of cases (see Helliwell TR:
Pathology of Bone and Joint Neoplasms. WB Saunders Co,
1999)
Available publications for the topic:
Leiomyosarcoma of bone
|

