|
|
|
|
|
Case #17
|
Typical Clinical Presentation:
|
|
A 27-year-old male presented with chronic, dull pain and some soft tissue swelling
along the antero-lateral surface of the left lower leg.
|
|
|
|
Characteristic Radiological Findings:
|
|
|

|
-
Plain film shows a large, cortically based, radiolucent lesion partially surrounded by a rim of
sclerotic bone, and two smaller lesions of similar appearance.
The location in the cortex of the tibial shaft is a major diagnostic clue (about 90% of these
tumors are centered in the antero-lateral cortex of the tibial shaft).
|
|
|
|
Pathological Findings: :
|
|
|
|
-
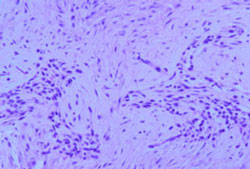
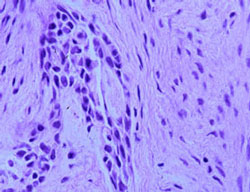
Biopsy material shows a moderately cellular fibrous stroma containing nests and strands of darkly
stained basaloid cells. Some nests demonstrated peripheral palisading reminiscent of basal cell carcinoma.
|
|
|
|
-
Both stromal cells and epitheliod cells are cytologically bland. There were no mitotic figures.
|
|
|
|
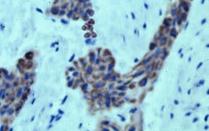
- Epithelial cells stain positive with cytokeratin AE1/AE3.
|
|
|
Diagnosis: Adamantinoma
|
|
Salient Points::
|
-
Adamantinoma is a rare, low-grade malignant neoplasm, which occurs almost exclusively in two skeletal
locations: the bones of the lower leg and the jaw. Tumors of the jaw are also known as "ameloblastomas".
Here, we will only discuss adamantinoma of long bones. Most patients are young adults, 20 to 30 years old.
-
Radiological appearance is very typical. In about 70% of cases the tumor involves the midshaft of the tibia
(Dorfman HD, Czerniak B. Bone Tumors. 1998). In the remaining cases, it is found at the ends of the tibia, and in
the fibula. Early lesions are characteristically centered in the anterolateral cortex. Advanced tumors may involve the medullary cavity and the soft tissues.
-
Histologically, the tumor consists of strands, nests, or large masses of epithelial cells
embedded in a fibrous stroma. The appearance of the epithelial cells and the cellular arrangement determine a histologic subtype: basaloid (shown above),
spindle, tubular, squamoid, and osteofibrous dysplasia-like.
-
Differential Diagnosis. Adamantinoma should be differentiated from metastatic carcinoma.
The location and radiological features help to separate the two. Characteristically,
epithelial cells of adamantinoma and stromal cells are bland with virtually absent (or very low)
mitotic activity. By immunohistochemistry, epithelial cells of adamantinoma are stongly positive for
cytokeratin. Cytogenetic studies usually reveal complex
chromosomal abnormalities involving multiple translocations and extra chromosomes.
-
Clinical Behavior. Despite its sometimes "benign" clinico-radiological appearance, adamantinoma
behaves as a low-grade malignant neoplasm characterized by local aggressiveness, high recurrence rate, and ability to
produce metastases. Metastases usually develop late in the course of the disease, in up to 25% of patients
(McCarthy EF, Frassica FJ. Pathology of Bone and Joint Disorders. 1998). The lungs are the most common site
of metastatic spread.
Available publications for the topic:
Adamantinoma
|
|
|

