|
|
|
|
|
Case #18
|
Typical Clinical Presentation:
|
A 16-year-old boy was seen in consultation for increasing pain in the mid upper arm.
Characteristically, the pain intensified at night and subsided with aspirin.
-
The effect of aspirin is an important diagnostic clue here.
|
|
|
|
Characteristic Radiological Findings:
|
|
|

|
-
Plain film shows a small, intracortical, radiolucent focus (nidus), surrounded by dense reactive periosteal bone.
The lesion is located in the mid portion of the humeral shaft.
|
|
|
|
Pathological Findings: :
|
|
|

|
-
If the nidus is removed intact, it appears as a circumscribed portion of red,
trabecular bone, usually less than 1cm in size.
|
|
|

|
-
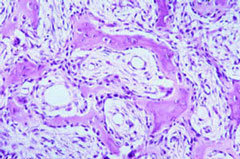
Low-power view shows the lesional tissue ("nidus"), well demarcated from the
surrounding sclerotic bone.
|
|
|
|
-
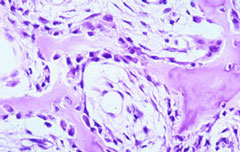
The lesion is composed of thin, often interconnected spicules
of osteoid and woven bone rimmed by osteoblasts. Osteoclast-like giant cells can be seen.
Intervening fibrous stroma shows prominent vascularity.
|
|
|
|
-
Both osteoblasts and stromal cells are without significant nuclear atypia.
|
|
|
Diagnosis: Osteoid Osteoma
|
|
Salient Points::
|
-
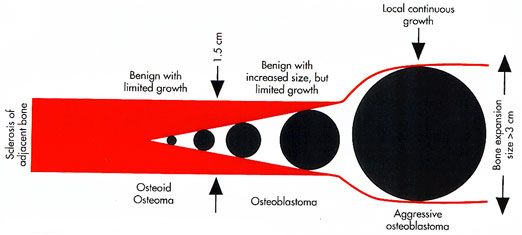
Osteoid osteoma is a common, benign, bone-producing neoplasm characterized by a small size,
limited growth potential, and a tendency to cause extensive reactive changes in surrounding tissues.
The lesional tissue, called a "nidus", usually appears as a small radiolucent focus, less than 1cm in size,
either within the cortex or adjacent to it. The lesion is thought to produce prostoglandin/prostocyclin-mediated
effects on the surrounding tissues inducing exuberant, reactive, periosteal sclerosis, soft tissue edema and pain.
Aspirin, which acts through inhibition of prostaglandin/prostacyclin, has dramatic pain-relieving effect in patients
with osteoid osteomas.
-
Predominant occurrence is in males between the ages of 10 and 25 years.
-
Location. Most frequently (50% of cases), osteoid osteomas arise in the femur and tibia.
The femoral neck is one of the most common anatomic sites. Other skeletal locations include the humerus,
the small bones of the hands and feet, and the spine. In a long bone, the tumor is usually found in the metaphyses
or diaphyses. If the lesion occurs in a close proximity to the articular surface of the joint, it causes severe reactive synovitis.
-
Precise localization of the lesion at surgery is difficult due to its small size and extensive reactive bone sclerosis.
Once the tissue has been removed, the pathologist should X-ray and thinly section the specimen to identify the nidus
(lesional tissue). Make sure the nidus is present. If not, contact the surgeon.
-
Differential Diagnosis. Osteoblastoma is a benign bone-forming neoplasm, which is closely related to osteoid osteoma.
Histological findings may be identical. However, remember that osteoblastoma is characterized by a larger size
(more than 1.5 cm) and absence of diagnostic clinico-radiological findings of osteoid osteoma.
Other important entity in the differential diagnosis is intracortical osteosarcoma. Look for the presence of
significant nuclear atypia and invasive growth pattern indicative of malignancy.
|
Reprinted with permission from Dorfman HD, Czerniak B: Bone Tumors. Mosby, Inc, 1998
|
|
|
|
Available publications for the topic:
Osteoid Osteoma
|
|
|

