|
|
|
|
|
Case # 20
|
|
An 11-year-old male was seen in consultation for an increasingly painful distal femoral lesion associated with a soft tissue mass.
|
|
Characteristic Radiological Findings
|
|
|

|
-
Plain radiograph shows an ill-defined destructive tumor in the distal femur. Fluffy
radiodense infiltrates represent malignant tumor osteoid.
|
|
|

|
-
MRI film delineates zones of bone destruction and soft tissue extension of the tumor.
|
|
Pathological Findings:
|
|
|
|
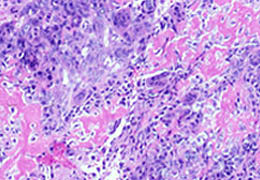
-
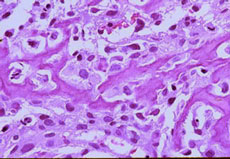
Biopsy material shows two major components of this neoplasm: highly pleomorphic cells and haphazard deposits of osteoid. Note that the malignant cells
fill the spaces between osteoid deposits.
|
|
|
|
-
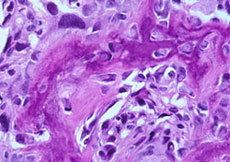
High magnification demonstrates anaplastic cellular features and mitotic activity.
|
|
|
|
-
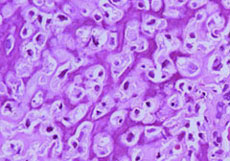
Lace-like osteoid deposition is very characteristic of this neoplasm.
|
|
|
|
-
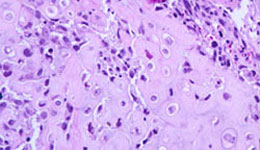
Few foci of neoplastic cartilage were present.
|
|
|
Diagnosis: Osteosarcoma, high grade
|
|
Salient Points:
|
-
Osteosarcoma is the most common primary sarcoma of bone. The peak incidence is in the
second decade of life during the period of the most active skeletal growth. Fewer than 5% of
osteosarcomas occur in children younger than 10 years (Dorfman HD, Czerniak B.
Bone Tumors. 1998). In elderly, osteosarcoma is usually seen in association with a pre-existing
bone disease, such as Paget's, radiation osteitis, or bone infarct.
By the time of presentation, all osteosarcomas are larger than 2 cm.
-
Location. In adolescents and young adults, osteosarcoma preferentially affects the most
rapidly growing parts of the skeleton: the distal femur and proximal tibia (50% of cases),
and the proximal humerus. Within the long bone, the metaphysis is the most common site.
In elderly, osteosarcoma tends to involve the axial skeleton and the flat bones.
-
Subtypes of osteosarcoma. Based on the location within the bone, osteosarcomas are
subdivided into intarmedullary, intracortical and surface osteosarcomas. Intramedullary,
or central, tumors comprise the largest group and include conventional high-grade
osteosarcoma, which accounts for about 90% of all osteosarcomas, and less common types
such as well-differentiated (or low-grade) osteosarcoma, chondroblastic, small cell, and
teleangiectatic osteosarcoma. Based on the degree of differentiation, osteosarcomas are
subclassified into high-grade and low-grade.
-
Pathologic diagnosis. Osteosarcoma is defined as a malignant tumor composed of neoplastic
mesenchymal cells synthesizing osteoid or immature bone. However, the histologic findings
can be extremely variable. For example, the tumor may appear identical to the MFH showing
minimal osteoid production, or it may contain masses of malignant cartilage, or numerous
giant cells. Remember that the presence of malignant osteoid distinguishes an osteosarcoma
from other sarcomas. Mineralization distinguishes osteoid from collagen deposits.
|
-
Malignant osteoid is deposited either in a lace-like pattern or in the form of haphazardly
arranged trabeculae of woven bone. Characteristically, the neoplastic cells fill the spaces
between the osteoid deposits and often become entrapped in osteoid. This is very
different from the reactive bone pattern, where the bone trabeculae are separated by a
fibrovascular stroma.
|
-
In cases of osteosarcoma, special techniques have been of little diagnostic help and used mainly to exclude other types of sarcoma.
-
Differential Diagnosis. In general, low-grade osteosarcoma should be differentiated from benign bone-producing tumors (osteoblastoma), whereas a high-grade osteosarcoma must be differentiated from other sarcomas. When you choose between benign and malignant, look for
the permeative growth pattern, cellular atypia, and mitotic activity. Also, examine the spaces between the bone trabeculae. In benign tumors they are occupied by a fibrovascular stroma. In osteosarcoma, they are filled with the aggregates of malignant mesenchymal cells.
The pattern of osteoid deposition is orderly in benign tumors and haphazard or lace-like in osteosarcoma. When you choose between an osteosarcoma and other types of sarcoma, look for malignant osteoid produced directly by mesenchymal cells.
-
Clinical Behavior. Conventional osteosarcoma is one of the most aggressive and highly lethal tumors. Prognosis depends on the skeletal site of involvement, surgical stage and tumor response to pre-operative chemotherapy. The most powerful predictor of outcome is the histologic response of the tumor to pre-operative chemotherapy. Tumor necrosis can be graded according to the following system (Rosen G, Caparros B, Huvos AG, et al. Preoperative chemotherapy for osteogenic sarcoma. Cancer 1982;49:1221-1230). Grade 1 - 0% to 50% necrosis; Grade 2 - 51% to 90%, Grade 3 - 91% to 99%, and Grade 4 - 100% necrosis. Data from MD Anderson Cancer Center shows that 90% and more of tumor necrosis is associated with nearly 90% 5-year disease-free survival, comparing to only 14% 5-year disease-free survival in patients with less than 90% of tumor necrosis (Dorfman HD, Czerniak B. Bone Tumors. 1998). Metastases, usually to the lungs, bones, and liver, are extremely common. Surgical resection of solitary metastases may improve the patient's survival (similar as for Ewing's sarcoma).
- Experimental data:
Abnormalities of the cell cycle regulating genes/proteins have been reported in different types of cancer. Inactivation of RB, p53, INK4A (encodes tumor supressor p16), and increased expression of CDK4 (cyclin-dependent kinase) and MDM2 have been reported in osteosarcoma.
Recent studies have shown frequent over-expression of Her2/neu by osteosarcoma and its correlation with a significantly worse histologic response to pre-operative chemotherapy and shorter event-free survival. Further studies are being conducted.
Recent studies have revealed the presence of SV40 (simian virus 40) genome in human malignancies (mesothelioma, osteosarcoma). It appears that SV40 integrates in human osteosarcoma DNA. Its role in the pathogenesis of osteosarcoma remains unclear
Available publications for the topic:
Osteosarcoma, high grade
|
|
Selected References::
|
- Gorlick R, Huvos AG, Heller G, Aledo A, et al. Expression of Her2/erbB-2 correlates with survival in osteosarcoma. J clin Oncol 1999;17(9):2781-2788
- Yamamoto H, Nakayama T, Murakami H, et al. High incidence of SV40-like sequences detection in tumour and peripheral blood of Japanese osteosarcoma patients. Br J Cancer 2000;82(10):1677-1681
-
Onda M, Matsuda S, Higaki S, et al: ErbB-2 expression is correlated with poor prognosis for patients with osteosarcoma. Cancer 77:71, 1996
|
|
|

