|
|
|
|
|
Case #3
|
Typical Clinical Presentation:
|
|
An incidental finding of a bone lesion in the distal femur of a 38-year old female. The lesion was completely asymptomatic.
|
|
|
|
Characteristic Radiological Findings:
|
|
|

|
-
Plain radiograph showed an intarmedullary zone of stippled and ring-shaped calcifications in the
distal femoral metaphysis. This mineralization pattern with radiodense stipples and rings is characteristic
of mature hyaline cartilage.
|
|
|
|
Pathological Findings: :
|
|
|
|
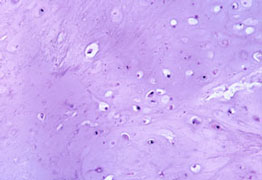
-
Low-power microscopic examination of the biopsy specimen shows three characteristic features
of this lesion: a) vague lobularity; b) abundant cartilaginous matrix, which can be
focally calcified; c) low cellularity.
|
|
|
|
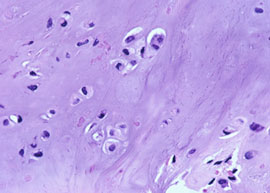
-
High-power view shows clustered and scattered chondrocytes with small, uniform, darkly stained nuclei.
Occasional bi-nucleated chondrocytes are present. Importantly, there were no mitotic figures.
|
|
|
Diagnosis: Enchondroma
|
|
Salient Points::
|
-
Enchondroma is a common, benign, intramedullary bone tumor composed of mature hyaline cartilage.
It shows wide age distribution with peak incidence during the third and fourth decades of life.
Characteristically, it has a limited growth potential and, therefore, many lesions remain
small and asymptomatic. Pain in enchondroma is a worrisome symptom, which indicates either a
pathologic fracture or continued growth. It is one of the criteria used to distinguish this
benign tumor from a low-grade (Grade 1) chondrosarcoma.
-
Location. In general, enchondromas are very rare in the sites most commonly affected by chondrosarcoma.
| Enchondroma
|
Characteristically involves the acral skeleton (small bones of the hands and feet - 60%)
and the long bones, such as femur, humerus, tibia, fibula, radius, and ulna). In the long bones,
the tumor is found in the metaphyses and proximal/distal diaphyses. Mid-shaft involvement is rare.
Enchondromas are very rare in the pelvis, ribs, scapula, and spine, and do not involve cranio-facial bones.
|
| Chondrosarcoma
|
Common in the pelvis, ribs, and long bones. Not unusual in the scapula, spine, and cranio-facial bones.
|
-
Differential Diagnosis. The difficult and important task is to distinguish an enchondroma from a low-grade (Grade 1)
chondrosarcoma. Histological differences are very subtle, and special studies are of no help.
Therefore, integration of clinical, radiological and pathologic findings is essential in making a diagnosis.
The presence of pain, large size of the lesion > 5cm, certain skeletal locations (see above) and "aggressive"
radiological features of the lesion favor the diagnosis of chondrosarcoma. Histologically, Grade 1 chondrosarcoma
shows moderate cellularity, mild nuclear atypia, "open" chromatin, small nucleoli, frequent bi-nucleated cells and rare
mitotic figures. Infiltrative growth pattern is indicative of malignancy.
-
Clinical Behavior. After the surgery, enchondromas typically heal. Recurrences are rare and should be carefully
evaluated for malignancy. The incidence of malignant transformation in a solitary enchondroma is low.
-
A rare, non-hereditary disorder characterized by multifocal proliferation of dysplastic cartilage is known as
enchondromatosis, or Ollier's disease. It is usually diagnosed in children and adolescents between 10 and 20
years of age. The risk of malignant transformation, usually to chondrosarcoma, is very high (20% - 30%).
For detailed discussion, see Dorfman HD, Czerniak B. Bone Tumors. 1998.
Available publications for the topic:
Enchondroma
|
|
|

