|
|
|
|
|
Case #5
|
Typical Clinical Presentation:
|
|
A 39-year-old female gave a 2-month history of increasing pain in her knee.
There was no evidence of joint effusion. Laboratory work-up showed normal serum levels of calcium,
phosphate and alkaline phosphatase.
|
|
|
|
Characteristic Radiological Findings:
|
|
|

|
-
Plain radiograph demonstrated a well defined, lytic lesion eccentrically located in the distal
femoral epiphysis with subchondral and metaphyseal extension. There was associated focal thinning of the cortex.
|
|
This is a very common radiological presentation of this tumor. Note the features of a slowly growing/locally
aggressive lesion: a geographic pattern of bone destruction with focal cortical erosion, and lack of a sclerotic rim.
Eccentric location in the epiphysis (with or without subchondral and metaphyseal extension) is another important
diagnostic clue.
|
|
|
|
Pathological Findings: :
|
|
|
|
-
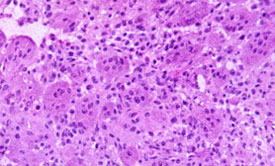
Curettage specimen consisted of fragments of soft, hemorrhagic, tan-brown tissue with some firm
areas and yellowish speckles. Microscopic examination showed a cellular lesion composed of
numerous multinucleated giant cells in a background of small, ovoid, mononuclear stromal cells.
|
|
|
|
-
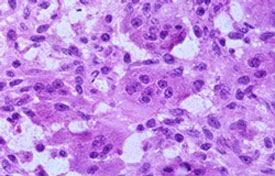
Stromal cells had poorly defined cytoplasmic borders and bland nuclei resembling those of
giant cells. Mitoses were easily found averaging 4 per 10 hpf. However, no atypical
mitoses were identified. Multinucleated giant cells resembled osteoclasts by their centrally
placed bland nuclei.
|
|
|
|
-
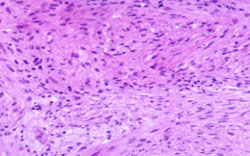
Some areas showed prominent fibrohistiocytic changes with storiform arrangement of
stromal cells and clusters of foamy histiocytes (xanthoma cells).
|
|
|
Diagnosis: Giant Cell Tumor of Bone (GCT)
|
|
Salient Points::
|
-
Conventional GCT of bone is a relatively common, locally aggressive neoplasm accounting for approximately
4% of all primary bone tumors. It affects skeletally mature individuals, F > M, 20 to 50 years of age. It is extremely
rare in children and patient older than 60 years. Histogenesis remains unclear. The cells of GCT have phenotypic
features of both macrophage-like (CD68 positive) and osteoclastic cells (immunoreactive with tartrate-resistant acid
phosphatase (TRAP), calcitonin and parathormone).
-
Location. Most GCTs affect the long bones with the highest incidence (65%) in the distal femur, proximal tibia and
distal radius. In the long bones, the tumor is invariably centered in the epiphysis. It can also be found in any other long
bone, pelvis and sacrum, and spine (3%). GCTs of the hands and feet are very rare.
-
Tumors that have radiological and morphologic features of GCT but are multifocal and/or located in the diaphyses
are unlikely to be conventional GCTs. Most often they are "brown tumors of hyperparathyroidism" found in patients
with abnormal serum levels of calcium and phosphate.
-
Certain histological features are inconsistent with the diagnosis of conventional GCT. These include marked nuclear
atypia and atypical mitoses in the stromal and multinocleated giant cells, as well as the presence of neoplastic cartilage
or malignant osteoid.
-
Note that in approximately 30% of cases, intravascular invasion is present. This incidental finding does not appear to
correlate with local aggressiveness or the development of pulmonary implants (see Dorfman HD, Czerniak B. Bone tumors.
1998). In a small number of patients, GCTs produce "benign", self-limited, non-invasive, pulmonary implants, which
are successfully treated by surgical excision.
-
Common secondary changes in GCT are hemorrhage and necrosis, fibrohistiocytic (xanthomatous) change, and
aneurysmal bone cyst formation. Complications include pathologic fractures and malignant transformation (dedifferentiation).
-
Clinical behavior. Conventional GCT is a locally aggressive neoplasm, which may produce bone destruction and soft
tissue invasion. Local recurrences are common (25% - 30%) and may involve bone and/or soft tissue.
The risk of local recurrence is related to radiologic stage rather than particular histologic
characteristics. Secondary malignant transformation, a rare complication seen mostly in
patients with prior irradiation, may be in the form of MFH, osteosarcoma or fibrosarcoma.
Primary de-novo malignant GCT is extremely rare and is characterized by marked
nuclear atypia of stromal cells and atypical mitoses.
Available publications for the topic:
Giant Cell Tumor of Bone
|
|
Selected References::
|
-
O'Donnell RJ, Springfield DS, Motwani HK, et al: Recurrence of giant cell tumors of the
long bones after curettage and packing with cement. J Bone Joint Surg 76A:1827, 1994
-
Kay RM, Seeger LL, et al: Pulmonary metastases of benign giant cell tumor of bone.
Six histologically confirmed cases, including one with spontaneous regression. Clin Orthop Rel Res
302:219, 1994
-
Fornasier VL, Protsner K, Zhang I, Mason L: The prognostic significance of histomorphometry
and immunohistochemistry in giant cell tumors of bone. Hum Pathol 27:754, 1996
-
Sanjay BKS, Sim FH, Unni KK, et al: Giant cell tumours of the spine. J Bone Joint Surg
75B:148, 1993
|
|
|

