|
|
|
Case #6
|
Typical Clinical Presentation:
|
A 14-year-old female was seen in consultation for an increasingly painful left humeral lesion
associated with mild joint effusion.
-
Pay attention to the patient's age, skeletal location, and the presence of joint
effusion, which may complicate epiphyseal lesions.
|
|
|
|
Characteristic Radiological Findings:
|
|
|

|
-
Plain radiograph showed an irregular, but circumscribed, lytic epiphyseal lesion surrounded
by reactive bone sclerosis. There was no evidence of bone expansion,
and the cortex was intact. The growth plates were open.
|
|
The clue here is the epiphyseal location of the tumor above the open growth plate,
and "benign" radiological features (good demarcation and a sclerotic rim).
|
|
|
|
Pathological Findings: :
|
|
|
|
-
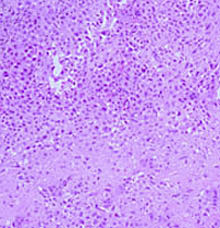
Curettage material showed a highly cellular tumor consisting of sheets of
round to polygonal cells. Multiple small foci of immature bluish-pink chondroid were present giving
a vaguely lobular appearance to the tumor. Many multinucleated giant cells were scattered
throughout the lesion.
|
|
|
|
-
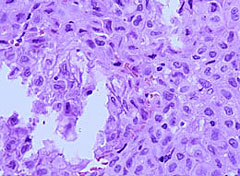
The cells were of intermediate size with folded, or clefted, nuclei,
fine chromatin pattern and occasional inconspicuous nucleoli. Mitotic activity was low.
|
|
|
|
-
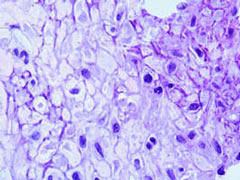
The cytoplasmic borders were very distinct with multiple foci of "chicken-wire"
calcification (calcified reticulin network around individual tumor cells).
|
|
|
|
-
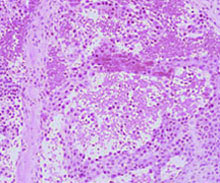
Few areas showed secondary cystic change.
|
|
|
Diagnosis: Chondroblastoma
|
|
Salient Points::
|
-
Chondroblastoma is a rare benign neoplasm occurring in 75% of cases
in the second decade of life, when the growth plates are still open.
This is one of two neoplasms of incompletely differentiated cartilage.
The other neoplasm is chondromyxoid fibroma.
-
Most common locations are the long bones (70% arise in the proximal humerus
and at the knee), and flat bones, including pelvis. In the long bones, the
tumor almost invariably occurs in the epiphysis.
-
The neoplastic round and polygonal cells are chondroblasts positive for S-100.
Multinucleated giant cells are of different cell line and stain positive for
histiocytic markers (CD68). "Chicken-wire" calcification is virtually
pathognomonic of chondroblastoma.
-
Secondary cystic change in the form of aneurysmal bone cyst is very common
20% - 30% of cases). This is most often seen in tarsal bones. Other types of
cystic change include formation unilocular or multilocular
cystic spaces filled with serous fluid.
-
Differential Diagnosis. Unlike chondroblastoma, Giant Cell Tumor (GCT) occurs in
skeletally mature individuals, lacks chondroid matrix, and shows negative staining
with S-100. Chondromyxoid fibroma is centered in the metaphysis and lacks calcification.
Clear cell chondrosarcoma, epiphyseally located malignant neoplasm, occurs in patients
older than 40 years and shows clearly malignant chondrocytes and the characteristic
large cells with clear cytoplasm.
-
Clinical behavior. Chondroblastoma is a benign neoplasm, which can
be successfully treated with curettage. Recurrence rate is about 10% within
the bone or in the adjacent soft tissue. Similar to GCT, chondroblastoma
can occasionally produce "benign", clinically non-progressive lung implants .
They can be successfully managed with surgery. The term "aggressive chondroblastoma"
is applied to large, locally destructive lesions, which may erode through the cortex
and invade the soft tissue. This behavior is relatively more common in pelvic lesions.
Available publications for the topic:
Chondroblastoma
|

