|
|
|
|
|
Case #7
|
Typical Clinical Picture:
|
|
A 22-year-old female was seen in consultation for a lesion in the proximal femur. She complained of chronic
mild to moderate pain in her right hip and was walking with a noticeable limp. Physical examination revealed
hip deformity and minimal limb length discrepancy. There were no other abnormal findings.
|
|
Characteristic Radiological Findings:
|
|
|

|
-
Plain film shows a large, elongated, well-defined intramedullary lesion of the proximal
femur with "shepherd's crook" deformity (lateral bowing) due to a healed
pathologic fracture. The lesion is partially surrounded by a sclerotic rim and has a
complex appearance with lytic areas, multiple foci of "ground glass" density, and radiopaque areas.
|
|
Note the intramedullary location of the lesion and its overall "benign" appearance evidenced by good demarcation,
geographic pattern of bone destruction and partial sclerotic rim. A very characteristic feature is
"ground glass" (homogenous) density. Remember that when this disorder involves the long bone, it commonly
produces what is called "long lesion in the long bone" with three key features: lucency,
sclerotic rim and cortical expansion.
|
|
|
|
Pathological Findings: :
|
|
|
|
-
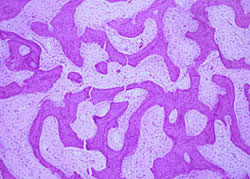
Curettage specimen consisted of pieces of firm, white-gray, gritty tissue. Microscopic examination showed moderately
cellular fibrous tissue with a whorled arrangement of bland spindle cells and interspersed,
slender, curved trabeculae of focally calcified woven bone ("chinese characters").
|
|
|
|
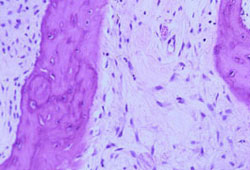
-
The majority of the trabeculae did not show an osteoblastic rimming or osteoclastic activity.
|
|
|
|
Remember three characteristic histologic features of this entity: a) thin, wavy spicules
of woven bone ("chinese characters"); b) lack of osteoblastic rimming or osteoclastic activity;
c) moderately cellular bland fibrous background. In children, stromal mitoses may be frequent,
1 to 5 per hpf. In adults, mitotic figures are very rare to absent.
|
|
|
Diagnosis: Fibrous Dysplasia
|
|
Salient Points::
|
-
Fibrous dysplasia is a common benign fibro-osseous lesion, which occurs sporadically during the period of skeletal
growth (ages 10 to 25). It is a hamartoma and is characterized by the intramedullary location. There are two forms
of the disease: monostotic (80% of cases) and polyostotic. Polyostotic involvement may be a part of McCune-Albright
syndrome (fibrous dysplasia, patchy cutaneous pigmentation, and precocious puberty), or Mazabraud's syndrome
(fibrous dysplastic lesions in close proximity to soft tissue myxomas).
-
Most common locations include the long bones (femur, tibia and humerus), the ribs, cranio-facial bones and pelvis.
In the long bones, the lesion is found in the metaphysis or diaphysis.
-
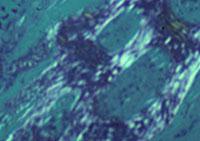
The hallmark of fibrous dysplasia is inability of tissue at the affected site to produce mature lamellar bone.
The maturation is arrested at the level of woven bone. The difference between the two types of bone is best appreciated
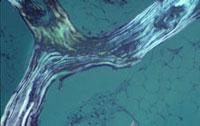
by using polarizing light.
|
-
Woven bone (immature bone) is characterized by random arrangement of the collagen fibers. In adults, this type of bone is only seen in
pathologic conditions such as fracture repair or bone-forming tumors. Keep in mind that
in benign conditions the bone trabeculae are surrounded by a fibrovascular stroma.
In malignant tumors, those spaces are often occupied by malignant cells.
|
|
|
|
-
In lamellar (mature) bone, the collagen fibers are orderly arranged forming
layers, known as lamellae.
|
-
Clinical behavior. Pathologic fractures and bone deformities are common complications. Occasionally,
lesions may show rapid enlargement due to secondary cystic changes including aneurysmal cyst formation.
Malignant transformation is a rare complication (less than 1%), more common with polyostotic disease.
Secondary malignancies are high-grade sarcomas (MFH, osteosarcoma, chondrosarcoma).
-
Differential diagnosis. Two important differential diagnoses include well-differentiated intramedullary osteosarcoma
and, in the tibia, osteofibrous dysplasia. Low-grade osteosarcoma is characterized by infiltrative growth pattern and mild
cellular atypia. Bone spicules are often rimmed by mildly atypical osteoblasts. Osteofibrous dysplasia can be ruled out based
on the intracortical location and orderly osteoblastic rimming of bone spicules.
Available publications for the topic:
Fibrous Dysplasia of Bone
|
|
|

