|
|
|
|
|
Case #9
|
Typical Clinical Presentation:
|
|
A 52-year-old female presented with an 8-month history of dull low back pain, mostly over the
sacrum, and recent onset of rectal pain and constipation. Her past medical history was non-contributory. |
|
|
|
Characteristic Radiological Findings:
|
|
|
|
-
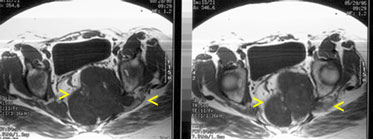
MRI film shows a large, destructive, sacral mass with lobulated margins and antero-lateral soft
tissue extension. The tumor appears to be centered in the midline.
|
|
The diagnostic clue here is the midline, axial location of the tumor. Also note "malignant" radiological features of the tumor evidenced by cortical destruction and a soft tissue mass.
|
|
|
|
Pathological Findings: :
|
|
|

|
-
Grossly, the tumor was multilobulated with glistening cut surfaces and soft to gelatinous
consistency. Extensive hemorrhages and necrotic areas were present.
|
|
|
|
-
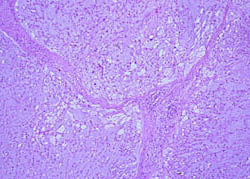
Low-power view shows characteristic lobular architecture.
|
|
|
|
-
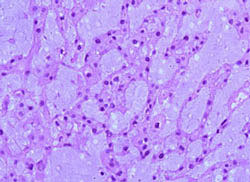
The tumor shows cord-like arrangement of cells and abundant myxoid extracellular matrix.
|
|
|
|
-
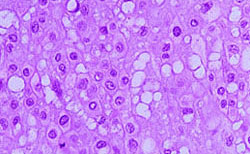
Two types of cells can be appreciated: smaller ovoid cells and the larger cells with numerous
cytoplasmic vacuoles. The latter are the hallmark of this tumor and are called
"physaliphorous cells". Occasional mitotic figures were identified.
However, no atypical mitoses were found. These tumors often demonstrate significant
cellular pleomorphism that is, probably, of no prognostic significance.
|
|
|
Diagnosis: Chordoma
|
|
Salient Points::
|
-
Chordoma is an uncommon, slow-growing malignant bone tumor, which is thought
to arise from the notochord remnants. Peak age incidence is between 55 and 65 years.
-
In 85% of cases, the tumor arises at either end of the notochord: in the sacrococcygeal(50%) or sphenooccipital(35%) regions. The remaining 15% involve the mobile spine.
-
Immunohistochemistry is a very helpful tool in the differential diagnosis of this tumor. Characteristically, chordoma shows positive staining with S-100 and epithelial markers (cytokeratin and EMA).
-
Two histologic variants are recognized: chondroid chordoma and dedifferentiated chordoma. Chondroid chordoma is a tumor containing a mixture of chordoid and cartilagenous elements. It seems to be associated with better prognosis. Dedifferentiated chordoma is a highly malignant biphasic neoplasm composed of typical chordoma and high-grade sarcoma. Use of immunostains usually helps to resolve diagnostic difficulties.
-
Distinguishing a chordoma from a large notochordal rest (benign remnant of notochord tissue) may be difficult. "These lesions are histologically and immunohistochemically identical. In this situation, only evidence of destructive growth can identify a chordoma" (McCarthy EF, Frassica FJ. Pathology of Bone and Joint Disorders. 1998).
-
Clinical Behavior. Chordomas are typically locally aggressive neoplasms, which because of their location may affect vital structures. With advanced tumors complete excision is difficult to achieve, and multiple local recurrences are typical. Distant metastases occur late in the course of disease and usually involve lungs, lymph nodes and skin.
- Experimental data:
There seem to be no correlation between the morphologic appearance of a tumor and the clinical course. As reported by Bergh et al, the only two histologial features that may have prognostic significance are microscopic tumor necrosis and Ki-67 labeling index >5%.
Cytogenetic analysis of chordomas shows no specific or characteristic chromosomal anomaly. Telomere elongation, microsatellite instability and loss of heterozygosity (LOH) have been reported in small series of cases.
Available publications for the topic:
Chordoma
|
|
Selected References::
|
-
Rosenberg AE, Brown GA, Bhan AK, et al: Chondroid chordoma - a variant of chordoma: A
morphologic and immunohistochemical study. Am J Clin Pathol 101:36, 1994
-
Wojno KJ, Hruban RH, Garin-Chesa P, et al: Chondroid chordomas and low-grade chondrosarcomas of the craniospinal axis. Am J Surg Pathol 16:1144, 1992
- Bergh P, Kindblom LG, Guntenberg B, Remotti F, Ryd W, Meis-Kindblom JM. Prognostic factors in chordoma of the sacrum and mobile spine: a study of 39 patients. Cancer 2000;88(9):2122-2133
- Klingler L, Shooks J, Fiedler PN, Marney A, et al. Microsatellite instability in sacral chordoma. J Surg Oncol 2000;73:100-103
|
|
|

