
Human Learning and Memory
Parkinson’s disease
Parkinson’s disease is a disorder involving progressive death of a certain type of neuron (brain cell) that produces the brain chemical dopamine. Patients with Parkinson’s disease show characteristic motor symptoms, including tremor and difficulty initiating movement. But more recently, research has documented additional cognitive symptoms in the disease: particularly difficulty in learning of new skills and habits. This appears to be due to the fact that the dopamine-producing neurons that are damaged in the disease also project to brain areas (such as the striatum) that are important for learning new habits and skills.
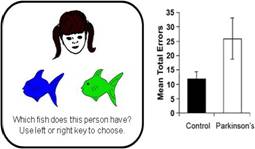
Left: In a simple test of learning and memory, participants view a series of faces on the computer screen and are asked to learn through trial and error which of two colored fish goes with each face. Right: Healthy adults (black bar) can learn these associations fairly quickly; patients with Parkinson’s disease are significantly slower. Adapted from Figure 2 of Herzallah et al. (2010) Cognitive and Behavioral Neurology, 23(2), 98-105.
It is thought that the brain uses subtle increases and decreases in the level of dopamine to help signal upcoming reward – making dopamine signalling particularly important in situations where a sequence of actions are needed to achieve a desired goal. As one example, (unmedicated) patients with Parkinson’s disease can be trained to play a computer-based “game” in which the goal is to accumulate as many points as possible. The patients are severely impaired at learning how to win points (reward-based learning), although they are as good as healthy controls at learning how to avoid losing points (punishment-based learning). This could be because the patients have reduced dopamine and therefore reduced ability to signal reward information in the brain.
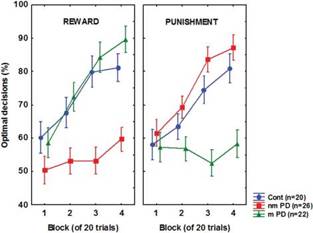 Parkinson’s disease – and its treatments -- affect cognitive as well as motor function. Unmedicated patients with Parkinson’s disease (red) are much worse than healthy controls (blue) on a task that involves learning through trial-and-error to obtain reward, although they are unimpaired on a task that involves learning to avoid punishment. This may be due to reductions in brain levels of dopamine in the patients. But when the patients are placed on medications that increase brain dopamine (green), they now show remediated reward learning – but severely impaired punishment learning. Adapted from Figure 2 of Nagy et al. (2007) Brain, 132:2385-2395.
Parkinson’s disease – and its treatments -- affect cognitive as well as motor function. Unmedicated patients with Parkinson’s disease (red) are much worse than healthy controls (blue) on a task that involves learning through trial-and-error to obtain reward, although they are unimpaired on a task that involves learning to avoid punishment. This may be due to reductions in brain levels of dopamine in the patients. But when the patients are placed on medications that increase brain dopamine (green), they now show remediated reward learning – but severely impaired punishment learning. Adapted from Figure 2 of Nagy et al. (2007) Brain, 132:2385-2395.
The most common medical treatment for Parkinson’s disease is use of drugs that help restore brain dopamine levels. Such treatment can often provide relief from the motor symptoms (although it does not stop the underlying progress of the disease). But if subtle increases and decreases in dopamine level are needed to help signal expected reward in the brain, then administering drugs that globally increase dopamine levels might actually impair learning – even while it ameliorates the motor symptoms. In fact, under many conditions this seems to be the case. For example, when patients with Parkinson’s disease are placed on dopaminergic medication, their motor symptoms decrease and they are no longer impaired at reward-based learning; but now, the medicated patients show a selective impairment at punishment-based learning. This could be because the dopaminergic drugs increase brain dopamine levels to a point where the subtle changes in dopamine level needed to signal upcoming expectations about reward and non-reward cannot be detected.
Parkinson’s disease is not the only syndrome in which dopamine is disrupted; schizophrenia, for example, is thought to involve increases in brain dopamine, while many drugs of abuse (including cocaine and amphetamines) act on the brain’s dopamine system. Understanding the dopamine system and its role in learning and memory will have implications for understanding all these syndromes. In addition, this research highlights the need for clinicians to consider cognitive, as well as motor, symptoms in evaluating the effectiveness of particular dopaminergic medications for their patients with Parkinson’s disease.
Representative Publications:
Herzallah, M. M., et al. (2010). Depression impairs learning while anti-cholinergics impair transfer generalization in Parkinson's patients tested on dopaminergic medications. Cognitive and Behavioral Neurology, 23(2), 98-105. Hyperlink to abstract: PMID: 20535058
Bódi, N., et al. (2009). Reward-learning and the novelty-seeking personality: A between- and within-subjects study of the effects of dopamine agonists on young Parkinson’s patients. Brain, 132(Pt 9):2385-2395. Hyperlink to free article: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2766178/?tool=pubmed
Vadhan, N., Myers, C. E., et al. (2008). Stimulus-response learning in long-term cocaine users: Acquired equivalence and probabilistic category learning. Drug and Alcohol Dependence, 93(1-2):155-162. Hyperlink to free article: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2247471/?tool=pubmed
Nagy, O., et al. (2007). Dopaminergic contribution to cognitive sequence learning. Journal of Neural Transmission, 114(5):607-612. Hyperlink to abstract: PMID: 17347774
Shohamy, D., Myers, C., et al. (2006). L-dopa impairs learning, but spares generalization, in Parkinson’s Disease. Neuropsychologia, 44(5), 774-784. Hyperlink to free article: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1626444/?tool=pubmed
Prior Funding: National Science Foundation, National Institute of Neurological Disorders and Stroke